Calgary's supervised consumption site by Central Memorial Park. Photo: Jeremy Klaszus
Sprawlcast Ep 20: This is a park for everybody
The realities of supervised consumption sites.

As Alberta's UCP government reviews supervised consumption sites, we look at what these places mean for the people who live in and around them.
A full transcript of the episode is below. You can subscribe to Sprawlcast on iTunes, Google Play or Spotify.
JEREMY KLASZUS (HOST): It's a warm September day, and 4th Street Southwest in the Beltline neighborhood of Calgary is bustling with life. On one side of the street is the Sheldon Chumir hospital; on the other side, Central Memorial Park, and today, the park is full of all kinds of people. A man in a suit leans against a wall reading a newspaper. Moms with strollers go by. By the library, arms and legs are waving in the air as a woman leads an exercise class of some sort.
VOICE: All right, bring those legs up. Starting off strong.
JEREMY: In the southwest corner of the park, five people are gathered together under a tree, including a young man who looks like he's asleep. His chin is resting against his chest. They are regular visitors to the supervised consumption site in the Sheldon Chumir across the street.
A couple cops on bikes pull up and the group starts to disperse, and as the cops rouse the young man, he starts to get upset. Pretty soon, he's crying – not just crying out, but crying – wailing. He thrashes backwards, and his head hits against the shopping cart behind him. He's in obvious distress and anguish.
It's hard to watch, and so people don't. They glance over at the commotion, then look away.

ROCCO: Yeah, he had gone to the site, and his drug of choice is the opiate, so he was falling asleep. It was putting him – you know, putting him out, and the officers obviously picked up on that and wanted to come over and see what was going on. That was their – that was their "in" to our group.
They didn't need to come and see us. He was just a guy falling asleep. There was no need to come and single us out.
JEREMY: This is Rocco. He's homeless, and he spends a lot of time at the park. He likes being close to the supervised consumption site, which is one of six that are operating in Alberta. These were put in place under the previous NDP government, and according to the Alberta Community Council on HIV, they have a 100% success rate.
In over 300,000 visits to these sites since they opened, no one has died from a drug overdose.
But the new UCP government has made it very clear that they're not keen on this service, and so they're reviewing it—and proposed new sites in the province have been put on hold.
This is a contentious issue, obviously. We're going to hear some different perspectives on it, starting with Rocco.
A safe place to go
ROCCO: I've been out of work for a little while. I got addicted to prescription painkillers, primarily. That's how this all began, and from there I ended up using non-prescription drugs that were a little bit harder than anything I've ever touched before. A lot of that's the crystal meth and a little bit of the fentanyl, but it's, I guess, the convenience in coming down here and being safe, first of all.
And it's a bit of a community too, right? You're in a group of your peers. You don't feel so in the shadows and alone, you know? So it's, in my opinion, a good program all around, despite the negatives that come with it.
JEREMY: And how long have you been coming to the site here?
ROCCO: I think I had my first visit was probably – well, just under – probably just under a year ago, and over that period of time, I've been drawn here more and more to, instead of – like, I'll walk here to use instead of just doing it wherever I am, and I kind of find that a little bit strange, but it's the social aspect of it.
It’s a bit of a community too, right? You’re in a group of your peers. You don’t feel so in the shadows and alone.
JEREMY: Yeah, definitely. And tell me a little bit more about that, because it is a medical facility, the supervised consumption site. It's a public health offering that's important, obviously. But that community aspect – I hear you saying that that's critical.
ROCCO: Well, especially for people like myself. Well, I guess I can't speak for anyone else, but we sort of live on the fringes of society with being – the majority of us are homeless. We're drug users, so what we have to do has to be done either behind closed doors, in the shadows – you know, you don't want kids to see you. You don't want – if you have any sense of responsibility at all, you don't want to be leaving remnants of your – what you've done out laying in a park.
I'm sure many people have seen it, and I've seen it myself. I can't believe that people leave what they leave hanging around after they've used. Like, it's disgusting, first of all, to see, and it's a health hazard for people, especially kids who aren't thinking about that.

JEREMY: Yeah. And is there a sense of ownership of this park by the people who are here?
ROCCO: You try to have some roots somewhere, because we have – being homeless, you have nowhere to plant yourself that you can safely call your own. We tend to try and make this a spot where we hang out, but honestly, we get run out pretty much – as you probably just witnessed there with what was going on when you arrived. We don't get much leeway, much freedom, as far as where we are and what we're doing. There were probably, within a 50-foot circumference of where we were sitting, there must have been 150 other people, and where did the law enforcement come?
JEREMY: Has that increased at all – when you think of even half a year ago or a year ago, in terms of the police presence?
ROCCO: With respect to contact? Yeah. And I'm not totally oblivious to what's going on for a lot of the people that – how they have to acquire what their – how they get their drugs. The neighbourhood has been a bit tense about what's been going on, and, granted, I get it. The police presence has been stepped up, so there's more guys around – of course the contact is going to be more frequent. I don't begrudge it.
I come from a family where my uncle was a police inspector, so I grew up with a lot of respect for the law growing up, and sometimes that's a detriment out here for me to have that type of respect and give them the leeway that they have, because everybody puts up barriers to – because they're afraid. Like you saw, that guy was crying his eyes out over there, so, it's a catch-22, depending on your own personal take on, I guess, law enforcement.
The neighbourhood has been a bit tense about what’s been going on, and, granted, I get it.
JEREMY: You mentioned, too how you're living on the margins of society. When you're in this park, do you feel that, or do you feel a part of what's all going on here in this beautiful park in the middle of the city, or do you feel kind of – yeah, what's the experience like?
ROCCO: Well, I certainly do. Like, I tend to – I still interact with the general public. I don't shy away as if I'm not one of them. I still am one of them, and when we're out in a park like this, this is a park for everybody, so there's no reason for us to feel ostracized, or even ostracize ourselves, when we're able to sit in a place like this and interact normally with everybody else in the city of Calgary. It's just, they may not be walking across the street to the consumption site like we might, but you're discreet. You're definitely discreet.
And that's all a certain – maybe a feeling of pride or whatever it is, but, you know, I wouldn't say, "Oh, well, I guess I'm going to run across the street and go do a shot now." Like, you keep that to yourself, because that's a habit that you have to have. It's what you have to do, and you don't broadcast it.
I still interact with the general public. I don’t shy away as if I’m not one of them — I still am one of them.
JEREMY: Yeah. And how would you describe the care that you get at the site over there?
ROCCO: It's incredible. They care way beyond what you would expect, especially when there's been either a close call or an overdose where they've had to do a reverse inside the building. The ladies – and the guys that are there, of course, too – they pay really close attention. They're making sure that if the person who was in distress is showing any other signs of potentially further distress or even something worse, they're right there. They're all over it. Yeah, they're amazing. It's great. I think they've – they've certainly saved lives. A hundred percent.
What if there was no SCS?
JEREMY: And what would it mean if that service wasn't there?
ROCCO: Sure, I want to say that the world's going to come apart and it's going to – all doom and gloom, but it's just going to morph or change, and we pivot and we do things a different way.
My feeling of safety for myself, I don't really push the envelope to the point where an overdose is imminent or potential, but I have friends who I worry about when they're out doing their thing, and I'm glad that they're supervised in the consumption site. If it's not there, I can't be there for them. I've saved 28 people, so, you know, I can't do it every – and I can't do it much longer, either. It's taxing.
JEREMY: What do you think people need to know about the crisis, as someone who's a user of the supervised consumption site? You know, you've been aware of the tension, like you describe, in the community, about having this service here. Yeah, what do you think people need to be aware of?
ROCCO: That the majority of the people that are in the position that they're in, whether they're using the consumption site or not – they may just be doing what they're doing outside of this facility. The majority of the people that are in this position are here because of a medical condition, and their ability to access prescription drugs to manage this – or at least mitigate it, and maybe even eradicate the addiction – they were taken away. They were cut off and had to go to another angle, which was, unfortunately, this fentanyl machine that's rolling around.
They care way beyond what you would expect, especially when there’s been either a close call or an overdose.
The majority of people that are down here are not people who went wandering into drug addiction eyes wide open and couldn't wait to get high. A lot of the people that are here and doing what they're doing, they're doing it because if they didn't, the sickness and the horrific experiences that you would have to go through are too scary to bear, and you go and you do this and risk your life every – like, you're risking your life every time you touch this shit. It's scary.
JEREMY: And how do you feel about your own outlook? You seem quite upbeat for somebody in the circumstance you're in.
ROCCO: Well, I'm still not even a hundred percent sure why I'm still here. I ended up here, and it was probably a – what really should have been a short-term thing, and I found a niche down here, and a sense of belonging, and maybe – I don't know, maybe a need down here for me and some of the things that I can do and – or I'm willing to do – and I feel I'm doing something that I should be doing, and maybe I'm punishing myself for something that I don't know what I did yet. I want out, but I don't think I'm ready yet.
JEREMY: Thanks very much for your time, Rocco.
ROCCO: Thank you.
Why are SCSs so contentious?
JEREMY: To learn more about this issue, I spoke with Rebecca Haines-Saah. She's an assistant professor in the Department of Community Health at the University of Calgary. Her training is as a health sociologist, and she's been looking at substance use, addiction, and harm reduction for two decades.

REBECCA HAINES-SAAH: I always make a little bit of a joke that harm reduction is so controversial that it can break up families, because even in my own immediate family, I have debates with folks that I love and care about who take a different approach than I do and find it hard to get on board with the idea of supervised consumption.
And I think it gets at the heart of the values that many of us were raised with – that it's better not to do drugs, or that people who use drugs make a choice, and if they become addicted or experience the consequences, well, they brought it on themselves. There's that sort of Judeo-Christian morality of being clean and being pure and being godlike.
And then on the flipside, there's almost a missionary-like zeal to save people in addiction, and that what we need to do to make them productive, healthy citizens – and contributing – is to get them clean and to get them off drugs and to force them into treatment or force them into jail.
And walking through the evidence that, although these are values that we've long held, the interventions based on these values don't really work, and they're not really effective. That takes a lot of either lived experience – direct experience – or a lot of convincing for some people. I think these are values that people hold on really tightly, and I always try and get back to the fact that, yeah, we all want really good outcomes for our family members, for the people we love.
There’s almost a missionary-like zeal to save people in addiction.
And the other thing is that in our homes and in our families and in our relationships with people, we've probably all been deeply impacted by substance use, addiction, and mental health. And so if you've had that experience growing up or you had a partner who struggled with addiction, or a child, you will likely have very strong views about the topic.
It's a very well-known idea in the literature and policy – the war on drugs. We say the war on drugs is actually a war on the people, right? So there's no war on the substance of cocaine, or there's no war on heroin. The war is on people using heroin and people using cocaine. These are the casualties. These are the people who feel the effects of the war – through incarceration, through overdose mortality, and through the sheer stigma of being socially excluded because you use drugs.
'Well-proven, but it is not benign'
JEREMY: In February, some frustrated residents and business owners took their concerns to city hall in Calgary. Here’s some of what was expressed to city councillors at that council committee meeting. The first speaker here is David Low with the Victoria Park Business Improvement Area, followed by Sherry Crawford.
DAVID LOW: Where we find ourselves today was formally being signalled by businesses and residents in the spring of 2018. Something was very wrong, yet concerns and warning signs were formally dismissed. Worse, the rhetorical device of “we are saving lives” was being used at every turn to instil doubt, guilt and anxiety over saying anything critical.
Good public health policy should not be crafted by rhetoric, value signalling or claims in the media. It needs to be based on facts, evidence and data. Yes, unequivocally, supervised consumption is well-proven, but it is not benign. There are serious consequences and impacts that need to be considered and balanced.
The rhetorical device of “we are saving lives” was being used at every turn to instil doubt, guilt and anxiety over saying anything critical.
SHERRY CRAWFORD: My daughter’s condo building has been broken into, and the neighbourhood now seems to be a magnet for all the crystal meth dealers and addicts in the city. I do have compassion for people struggling with addiction. I volunteered at the Calgary Young Offenders Centre for eight years, and I know some of the horrors that people do try and forget through drugs. I’ve also had a good friend die through drug use.
I do think every life is of value and every life matters. However, in order to reduce the harm that addicts do to themselves, you knowingly and deliberately choose to put the lives of all the innocent, tax-paying, contributing members of society who live there at risk.
JEREMY: The next speaker was Jessica McEachern, a peer support worker for the SCS.
JESSICA MCEACHERN: The hyper-vigilance I feel like has been created ever since this—people are trying to find a reason to shut us down. People want a reason, and now they’re finding it in meth users. But I was a meth user, and now I’m a contributing member of society. It’s possible. We can’t punish people out of this. We can’t criminalize our way out of this. I understand people feel scared of people they don’t understand and know.
And I also want to say that people with meth psychosis—I’ve been in meth psychosis—they are terrified. They are paranoid and extremely terrified. They are not angry, they’re not hostile. They feel like everything is—like they’re going to get arrested. They feel like everything is coming down on them, everybody’s in on it and they’re just terrified and scared.
JEREMY: Some of the people who spoke out at that meeting say that they’ve seen an improvement now that there’s more police in the area. I asked Rebecca Haines-Saah about this. Is opposition to these sites based in legitimate concerns about safety or does it have more to do with discomfort with people who are marginalized?
Sanitizing the inner city
HAINES-SAAH: I think the assumption that everybody is necessarily disorderly and violent is informed by fear, and this is something strong for me to say, but I really feel it deeply, having grown up in a marginalized community in Toronto, which is Regent Park, is that people have a lot of assumptions about living in a so-called "drug neighbourhood," and I really balk at the idea that people in downtown want a downtown urban condo lifestyle, but want it completely sanitized.
And I'm not saying people need to live in a context where they feel unsafe or where there's crime, but inner cities have crime. Crime is up across our city. It's not only because of the supervised consumption site. So I feel like it's being scapegoated. And this mainly comes when people say, "Oh, well, if you are such a strong advocate for safe consumption sites, Rebecca, why don't you put it in your community?" Well guess what? I grew up in a community where drug use, drug selling, sex work, was happening not far from my doorstep, so I have experienced that. It really wasn't a threat to my safety, and it actually made me more compassionate and want to work in this area.
I don't want to be dismissive, and I don't want to sound patronizing to community members who have concerns, but you read comments where people say, "I was walking with my kid to school in the Beltline, and we were playing a game called 'count the needles.'" Now, I've walked around the Beltline. I've seen some needles, occasionally. I wouldn't say there's enough to play "count the needles," and I really question what parent would actually find that to be a fun game with their kids.
I've heard other adults say they're afraid to even go to the Chumir site. I have been there for urgent care getting stitches in my leg, and I didn't feel at risk at any time. There's a lot of security there. If anything, that model of a supervised consumption site is very corporate and very different from other models, right? There's lots of security, and it's in a well-lit, very safe building.
I really balk at the idea that people want a downtown urban condo lifestyle, but want it completely sanitized.
So yeah, there's that idea that kids are necessarily at risk, and what are we communicating to our kids? I'd like to ask people, and this – a doctor who works in harm reduction in the US, Aaron Fox, has made this point – what message are we sending to our kids if we allow citizens to die of overdose, right? Isn't it a message that we don't care about people using drugs if we're not doing everything we can when two people a day are dying of opioid-related overdose, right?
JEREMY: Mm-hmm. And let's talk about that – what these supervised consumption sites do day in and day out, 24 hours a day. Yeah, what is the impact? I think that's something that gets lost, because the, kind of – the superficial version is they go there and they use drugs, and then all these kind of judgments kick in that, as you say, we're kind of raised with from very early on.
HAINES-SAAH: Yeah. Well, I think on one level, there's this idea that we're enabling drug use, we're encouraging drug use, or we're attracting people to the site. And that is counterintuitive to the needs assessment that was done by my colleagues here at the University of Calgary that showed people using drugs downtown and in our neighbourhoods would not travel more than about 1.1 km to use drugs, right?
So the services were put with a – were put because there was a need there, so the idea that if they weren't there people wouldn't be using drugs downtown and they wouldn't be intoxicated in public or maybe littering or sometimes getting in fights or self harming and being frightening to people – I think that's a myth. These are problems we have to grapple with, and I know that services such as the [Alpha House] DOAP Team were scaled up to try and address some of the needle debris and some of the disorder.
We know from the literature that this takes time. It takes up to five years for people to feel like, ‘Okay, this is acceptable in our community.’
One of the other things that is really hard to grapple with is that in response to community concerns, police presence was scaled up around the site, and from what we know from people using drugs, that's a real deterrent to using the site. So it is, I think, a challenge for community to accept, but we also know from the literature that this takes time. It takes up to five years for people to feel like, okay, this is acceptable in our community.
So when I – I've commented on social media when I see these police reports about calls to police are up, you know, check on welfare, reports of disorder are up. I think this has a lot to do with hypervigilance in the community and people really watching and being concerned and having a low tolerance, and I just think all the energy put into observing and monitoring and fighting and protesting—we could put this towards community-based solutions. We could think about ways to work with existing organizations that are supporting people, and we could expend that energy in a better direction.
But again, we're in this place of deep denial about substance use problems, and, kind of, blinders, about what's really going to work. The idea that if we got everyone into detox they'd get clean and they'd get a job and they'd carry on with their life – that's a great goal, but it's not what's appropriate for everybody.
The UCP review
JEREMY: And the province right now, they've set up a panel to look at these supervised consumption sites and do a review. What's your sense of that panel and that entire effort?
HAINES-SAAH: Well, when talk of the panel first started coming out in June, I immediately got anxious and worried seeing that, from the get-go, the emphasis was on the socio-economic impact, and this is not typically the markers or the metrics of how we evaluate a public health intervention or a healthcare service.
Now, social disorder is something that we need to look at, but the evidence we have across North America has not shown consistently that these increased drug-related crime and disorder. So the government saying they have the public health evidence in their possession, and we've already looked in the last government at the harm reduction literature, so this is going to do something new. All that's going to be out of scope, and we're going to look at the impact on businesses and communities.
Well, I feel like when you generate that evidence, it is catering to the people who've been unhappy with it. They're going to come out; they're going to say what they didn't like. What will be the way of deciding what wins out in the end? Are we going to count the number of people who said they dislike it, or it's had an impact on their business, versus the community members who say they have no problem with it? And how are we going to weight that evidence in a really unbiased and objective way against the public health evidence around the positive benefits?
So I'm not saying that these sites are perfect, and I'm not saying that there aren't things that we could improve upon, or that everybody should accept them. But to me, it seems like an exercise in futility, and like the decision has already been decided.
Many are the casualties of our economy, right? They’re casualties of this inequity in society.
And then I'll say one other thing in that. There is a great emphasis, also, on this idea that we need to invest in treatment and we need to invest in the continuum of care. And I've been working in drug policy and mental health – it pains me to say, but it's been 20 years now, in three different provinces, and the continuum of care is a wonderful idea. It's a concept around which we've had so many consultations and stakeholder tables and government engagement, and we don't have a continuum of care.
It would be nice to think that this government is going to implement this beautiful, wonderful continuum of care for people with addictions. I'm very skeptical that could happen, and the fact that that's being sold as a solution that's going to be better than harm reduction, that harm reduction is only a tiny part of the continuum of care and we're going to expand it and it's going to be great – we have a Valuing Mental Health Report that's recommended this already – wasn't acted on by our last government. I think it's unrealistic.
So when you hear that rhetoric that, well, we need to invest more in treatment and the continuum of care solution, it's really a lot of rhetoric, you know?
JEREMY: When you look at the news about this, and kind of the public conversation around supervised consumption sites, what do you think is missing from the conversation?
HAINES-SAAH: I think what's missing from the conversation, from someone who is a sociologist and someone who looks at – in public health, at what we call the structural context in health inequities, is that the solutions are bigger than treatment and harm reduction. The solutions are really looking at root causes and providing people with jobs and with stable housing and with meaningful lives – all those supports and services.
So the idea that you can live in a city with incredible wealth, such as ours, and such a gap between the rich and the poor, and so many people making so much money and it not really being fairly distributed to other people – these people who are suffering, who are underhoused, and who have addiction and mental health issues, and who are living on the streets, many are the casualties of our economy, right? They're casualties of this inequity in society.
And so as we continue to profit, we're further harming them by saying they need to get off drugs so they can also contribute to our economy. I'm going to sound like a socialist, but it is a critique of capitalism, and it is a critique of inequity.
The debate in Lethbridge
JEREMY: We're going to come back to that interview. But first, let's go to Lethbridge, because this issue of root causes is one that came up at a city council meeting there in August. Here's Lethbridge Mayor Chris Spearman.
MAYOR CHRIS SPEARMAN: The supervised consumption site has certainly had challenges in the community. It's a new facility in a smaller city. But we have root causes for the drug issue – root causes that are things like poverty and homelessness and unemployment. And people who are on drugs, who are addicted, often say their life on drugs is better than the life off of drugs, because we're not dealing with the root causes.
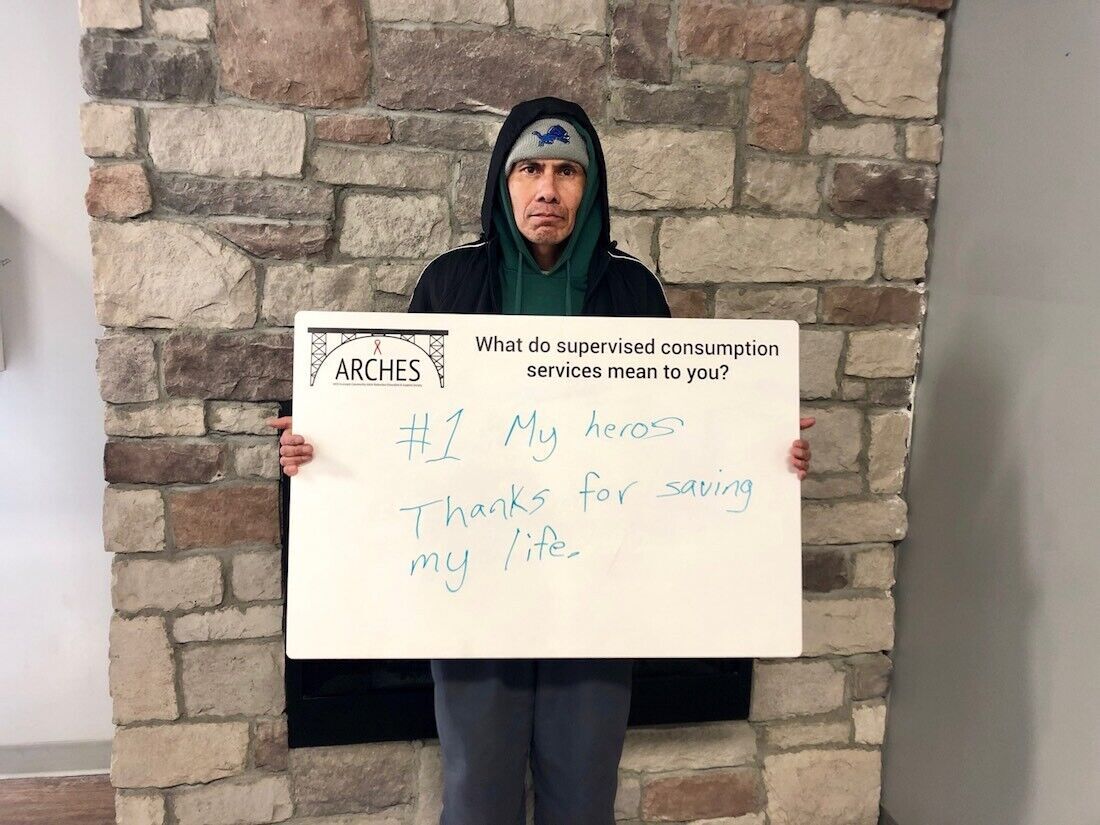
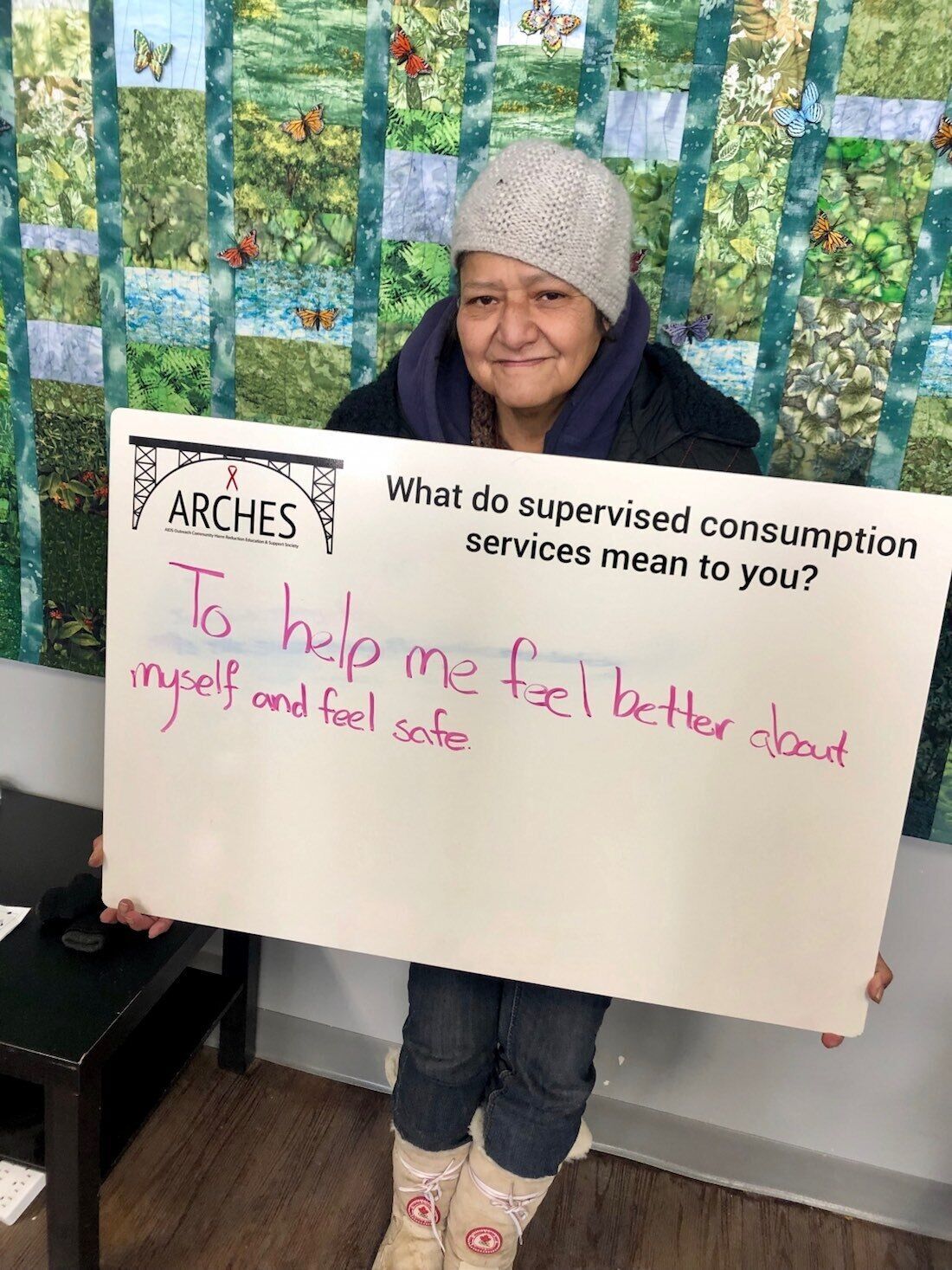
JEREMY: The Lethbridge supervised consumption site opened in early 2018. It's run by a nonprofit agency called ARCHES. Councillor Blaine Hyggen put forward a motion for Lethbridge's city council to ask the province to defund the supervised consumption site.
Now, this council meeting happened on the same day that the UCP government announced its new panel to review supervised consumption sites around the province. Let's listen in to a bit of this debate. We're going to hear from Councillor Hyggen, followed by Councillor Joe Mauro, who also supported the motion.
I want them off drugs. I want them clean and healthy. I want them to be part of our society.
COUNCILLOR BLAINE HYGGEN: People have said on social media that I must hate drug users and I want them to die, because I'm against the SCS. I don't hate them. I have compassion for them. I don't want them to die. I don't want to be enabling – and, indeed, encouraging them – to stay on drugs. I want them off drugs. I want them clean and healthy. I want them to be part of our society. I want them living life to the fullest potential with friends and a sense of purpose.
COUNCILLOR JOE MAURO: Great news from the government today. I think we're all happy, and I think we all expect that. But the nine of us here aren't representing the province of Alberta – we're representing our community.
And so if we were to pass this resolution, I think it would send a message to the province, clearly, of how we, as a nine members of council, we've heard our community. We hear their frustrations, whatever else they've shared with us. To me, this is the appropriate time to do it, because they would understand that the nine of us here are listening to our community, trying to resolve their problems—and we can't.
JEREMY: Now we'll hear from Councillor Rob Miyashiro, followed by councillors Jeff Coffman and Belinda Crowson.
Defunding the supervised consumption site will mean people die.
COUNCILLOR ROB MIYASHIRO: This'll be really succinct, after hearing that. Councillor Mauro, do you want people in Lethbridge to die? Our most marginalized population – do you want them to die?
COUNCILLOR MAURO: Councillor Miyashiro, I'll –
COUNCILLOR MIYASHIRO: Yes or no?
COUNCILLOR MAURO: I'll let you answer that.
COUNCILLOR MIYASHIRO: No, I'm asking you. Do you want our most marginalized population in Lethbridge to die?
COUNCILLOR MAURO: Councillor Miyashiro, I'll let you answer that. You know the answer.
COUNCILLOR MIYASHIRO: Well, defunding the supervised consumption site will mean people die. So thank you for your answer.
COUNCILLOR JEFF COFFMAN: A friend of mine actually recently said that the one thing that she's noticed about this debate, or this conversation, is that we seem to be a community that's losing empathy. We're losing empathy for those struggling with addictions, mental health, homelessness. We're losing empathy for those who are investing in the community, dedicating themselves to producing goods and services, creating a living.
What's also coming out of it is that we're starting to vilify people. We're starting to vilify people in the business community because they are frustrated, they are angry, they are worried. And we're vilifying a not-for-profit organization who is trying to actually do something during this crisis, and that really, really concerns me, because that's not the way a good community moves forward.
COUNCILLOR BELINDA CROWSON: I have sat with every member of this council on committees and on groups trying to solve this in various ways. I know people's hearts are in this and want to do better, and what keeps me grounded and keeps me moving forward, when I actually get off social media – and I'd recommend you all get off social media – and we actually talk to people in Lethbridge, it quickly becomes obvious how much more we have in common and how much we are thinking similarly on this issue.
And what is absolutely incredible, today we have focused on the one thing that is separating us. Let's start talking about what we have in common. We are facing a drug epidemic in Lethbridge and across North America. When you are facing a complex issue, you need complex, coordinated answers to that issue. We need answers from public health, recovering treatment, police, from the judicial system, from governance, from housing, and we need them to work in a coordinated fashion. Not only are we not seeing enough resources, we are not seeing a systemic approach to this.
Let’s be clear about this: We’re in an epidemic. Epidemics need smart public health decisions made by public health experts.
Be very aware: The supervised consumption site is not our jurisdiction. It was licensed by the federal government, and it is funded through the provincial government. But when it comes to the supervised consumption site, when it comes to its role in harm reduction, I approach it as I will when we look at vaccines in a month or so as the flu vaccines come out – I look to the public health experts. Because, again, it's not our jurisdiction, so I look to experts to help us figure it out.
We see, with the increase in measles and the epidemics related to other contagious diseases, what happens when even the best intentions lead to fear and misinformation which influence public health. Diseases we thought we had put behind us are once again prevalent, and kids are again put in danger.
Let's be clear about this: We're in an epidemic. Epidemics need smart public health decisions made by public health experts. We also, of course, need the experts to help us in addictions recovery policing. These aren't the only answers, but they are vital parts of the answers. I will not support this resolution. I will support my city, as I've done for years. I will continue to fight for everyone in this city. I'll advocate, I'll promote, I'll work with anyone who wants to build a better Lethbridge, but I will not go backwards. Thank you.
JEREMY: Councillor Hyggen's motion was voted down 6-3, which means the Lethbridge supervised consumption site will keep serving the people who need it – at least, for now.
All right, let's go back to that interview with Rebecca Haines-Saah at the University of Calgary.
What changes people's minds?
JEREMY: I'm curious – in the course of your work, have you, like – have you observed what makes people change their minds about harm reduction? Because it is a bit of a process for a lot of people.
HAINES-SAAH: I think it's really interesting. So, on a communication level, I think face-to-face conversations – a podcast like this, or the conversation you and I are having. Or even, you know, I've had radio interviews with journalists I would say are on the conservative side, and to see them shift their views and to see them support harm reduction conversations because they hear the evidence. And also, you know, having that family experience or hearing from family members sometimes shifts people.
I'm struck, though, that there is a lack of compassion, because I do have research with parents whose children have died from overdose, and sometimes I see and hear comments like, well, there must be something wrong with that family that their kid used drugs, and if you were a better parent, maybe your child wouldn't have died. So there are some people who lack compassion and lack understanding, and I don't think we can change them. But I think face-to-face conversation does a lot. You can't bombard people with evidence, and, you know, I think it's on public health folks and academics – we love to bombard people with evidence. It doesn't really change hearts and minds all too well.
People forget that it’s based on compassion and it’s based on meeting people where they are at.
And then the other thing, of course, that changes how people think and feel is whether or not the substance is illegal, right? So a lot of people will – I mean, it's a good thing that we're invested in the social contract, and, we – a lot of people are focused on obeying the law and keeping that civil discourse. But I've seen that with my work on cannabis, right? So as cannabis was legalized, many people started to shift their views and say things like, "Well, lots of people are already using it. I totally agree it should be legal. I just don't want to see corporations take over and make a lot of money or more people start to use or kids having problems."
So I think that illegal status of the substances being used has a lot to do with it? Pundits or people just joking in the harm reduction area will say, you know, bars are safe consumption sites, and they're accepted in every community. They lead to disorder and public urination and violence and other types of things, but we accept them as part of our community where people are going to go and get messed up and use substances, right?
JEREMY: Yeah, it's very socially acceptable, and even encouraged. You're supposed to do that.
HAINES-SAAH: Right. Right. So alcohol use is okay, but we put some parameters around that to try and keep people safe, in terms of how we distribute it, having a safe supply, protecting minors, and not drinking and driving. So I think the legal – the criminalization and stigma has a lot to do with it.
I want to remind people that harm reduction is not just supervised consumption sites. It started in a style of intervention with needle exchanges, but it is a suite of interventions, and an approach that, I think – people forget that it's based on compassion and it's based on meeting people where they are at, and that at every stage of drug use, or at every stage of life, we can improve someone's quality of life and day-to-day existence. And more so than that, we can make them feel like they matter. Like when I come into this place, people respect me, they want to help me, they're there for me, and they're not judging me.
Beyond that, in the bigger picture, we have an ethical imperative to provide universal healthcare to people, regardless of the behaviour that they're engaging in. And if we're going to apply that to people who are using drugs, you can see how you can easily apply that idea that some people don't deserve care to people who are inactive, or people who are obese, or people who are engaging in any range of behaviours that put themselves at risk, and whoever is making those decisions about what's in and what's out.
So there is that idea of compassion and caring and connecting people and telling them that they matter, but also that above and beyond that, it's part of their rights as citizens to receive healthcare.
JEREMY: Well, thanks very much for your time and insight, Rebecca.
HAINES-SAAH: Thanks very much.
Jeremy Klaszus is editor-in-chief of The Sprawl.
Note: ARCHES Lethbridge clients gave consent for their photos to be taken and shared by the agency.
The Sprawl is crowdfunded, ad-free and made in Calgary. To do local journalism like this, we rely on members who kick in a few dollars a month. Become a Sprawl member today to support independent Alberta journalism!
Support independent Calgary journalism!
Sign Me Up!The Sprawl connects Calgarians with their city through in-depth, curiosity-driven journalism. But we can't do it alone. If you value our work, support The Sprawl so we can keep digging into municipal issues in Calgary!